For More
Information
Lower respiratory tract infections can present in many different ways, including acute bronchitis, community-acquired pneumonia, and acute exacerbation of chronic obstructive pulmonary disease.
In the past, this ambiguity was met with almost-automatic antibiotic therapy. Today, we have better information and better ways to decide if antibiotics are warranted.
For More
Information
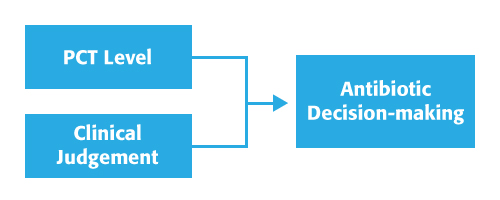
Procalcitonin (PCT) provides critical biomarker information. PCT is produced by numerous organs at a cellular level after bacterial pro-inflammatory stimulation.1,2
Procalcitonin is a host response to bacterial insult.3-5
Viral Infections inhibit PCT expression, enhancing the ability to distinguish bacterial infections from non-bacterial infections (PCT is not specifically indicated as a viral marker).
For patients with suspected or confirmed lower respiratory tract infection (LRTI), defined as community-acquired pneumonia (CAP), acute bronchitis, and acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
| PCT Value | <0.1 ng/mL | 0.1 - 0.25 ng/mL | 0.26 - 0.5 ng/mL | >0.5 ng/mL |
| Initiation of Antibiotic Use Recommendation | Strongly Discourage | Discourage | Encourage | Strongly Encourage |
| Clinical Considerations |
|
|
||
| LRTI | ||
| PCT Value | <0.25 ng/mL | ↓ >80% from peak |
| Discontinuation of Antibiotic Use Recommendation | Encourage | |
| Clinical Considerations |
|
|
Significant reduction in antibiotic initiation
Significant reduction in exposure to antibiotics
No adverse safety signals associated with PCT guidance for LRTI
For more information, please see full package insert for VIDAS B•R•A•H•M•S PCT (30450-01).
In conjunction with clinical assessments, use of PCT can increase accuracy of early diagnosis and enable more appropriate clinical decisions.
In just 20 minutes, you can get results from a proven, sensitive biomarker that provides specific information that adds to physician acumen, and enables more appropriate triage decisions.
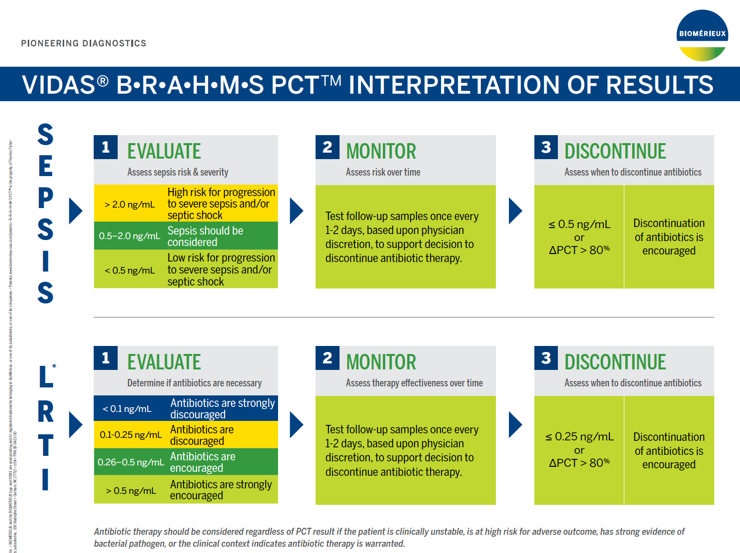
| >2.0 ng/mL | High risk for progression to severe sepsis and/or septic shock |
| 0.5 - 2.0 ng/mL | Sepsis should be considered |
| <0.5 ng/mL | Low risk for progression to severe sepsis and/or septic shock |
Assessing PCT values over time provides valuable information regarding patient disposition, response to treatment, and likelihood of survival.
Follow up samples should be tested once every 1-2 days, based upon physician discretion to support decision to discontinue antibiotic therapy.
VIDAS B•R•A•H•M•S PCT has been cleared by the FDA to aid in decision making on antibiotic discontinuation for patients with suspected or confirmed sepsis.
Discontinuation of antibiotics is encouraged if the PCT concentration is ≤0.50 ng/mL or if the ∆PCT >80%.
Antibiotic therapy may be continued based upon other clinical findings, such as failure to control a local infection, or ongoing physiologic instability.
For Critically Ill Patients:
So you can achieve the goal of giving antibiotics to the right patients, at the right time, for the right duration.
Clinical Guide to Use of Procalcitonin
VIDAS B•R•A•M•H•S PCT Wall Chart
VIDAS® 3 is a benchtop immunoassay system designed specifically for low throughput testing. Fully automated, it is based on the proven and robust ELFA technology that makes VIDAS a gold standard worldwide for high quality on-demand test results.
Visit VIDAS B•R•A•H•M•S PCT |
Visit VIDAS 3 |
Order Online |
References: